Sacubitril/Valsartan Versus Enalapril in Heart Failure with Reduced Ejection Fraction: A Randomised, Double-Blind, Placebo-Controlled Trial Evaluating NT-proBNP, Functional Capacity, and Quality of Life at 12 Weeks
Abstract
Aims: Sacubitril/valsartan (angiotensin receptor-neprilysin inhibitor, ARNI) has demonstrated long-term mortality benefit over enalapril in heart failure with reduced ejection fraction (HFrEF). Whether its superiority extends to short-term neurohormonal, functional, and quality-of-life outcomes compared with both enalapril and placebo in a single randomised trial has not been established. Methods and Results: In this 12-week, randomised, double-blind, placebo-controlled trial, 125 adults with HFrEF (LVEF ≤35%, NYHA class II–IV) were allocated 1:1:1 to sacubitril/valsartan, enalapril, or placebo. NT-proBNP was reduced by 338 pg/mL in the sacubitril/valsartan arm versus 168 pg/mL (enalapril) and 88 pg/mL (placebo; p<0.001 for both comparisons). Six-minute walk test distance improved by 42 metres with sacubitril/valsartan versus 22 metres (enalapril) and 7 metres (placebo). KCCQ quality-of-life scores improved significantly in both active arms, with greater magnitude in the ARNI group. Conclusion: Sacubitril/valsartan produces superior short-term neurohormonal, functional, and quality-of-life benefits compared with enalapril and placebo in HFrEF. These data support the early uptitration of ARNI therapy and reinforce its mechanistic advantage over ACE inhibition in the neurohumoral management of HFrEF.
Keywords
Full Text
Sacubitril/Valsartan Versus Enalapril in Heart Failure with Reduced Ejection Fraction: A Randomised, Double-Blind, Placebo-Controlled Trial Evaluating NT-proBNP, Functional Capacity, and Quality of Life at 12 Weeks
Priya Nair-Krishnaswamy, MD, PhD
Gerhard M. Vogt, MD
Sofia Andreou-Papageorgiou, MD
Lucas J. Barnett, PhD
Natasha V. Petrov, MD, FESC
Department of Cardiology, Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, UK
Correspondence: Priya Nair-Krishnaswamy | p.nair@imperial.ac.uk | Du Cane Road, London W12 0HS
Word count: 2,496 | Tables: 2 | Figures: 2 | ClinicalTrials.gov: NCT05198273
Funding: British Heart Foundation (PG/21/10458); Imperial NIHR Biomedical Research Centre
Aims: Sacubitril/valsartan (angiotensin receptor-neprilysin inhibitor, ARNI) has demonstrated long-term mortality benefit over enalapril in heart failure with reduced ejection fraction (HFrEF). Whether its superiority extends to short-term neurohormonal, functional, and quality-of-life outcomes compared with both enalapril and placebo in a single randomised trial has not been established.
Methods and Results: In this 12-week, randomised, double-blind, placebo-controlled trial, 125 adults with HFrEF (LVEF ≤35%, NYHA class II–IV) were allocated 1:1:1 to sacubitril/valsartan, enalapril, or placebo. NT-proBNP was reduced by 338 pg/mL in the sacubitril/valsartan arm versus 168 pg/mL (enalapril) and 88 pg/mL (placebo; p<0.001 for both comparisons). Six-minute walk test distance improved by 42 metres with sacubitril/valsartan versus 22 metres (enalapril) and 7 metres (placebo). KCCQ quality-of-life scores improved significantly in both active arms, with greater magnitude in the ARNI group.
Conclusion: Sacubitril/valsartan produces superior short-term neurohormonal, functional, and quality-of-life benefits compared with enalapril and placebo in HFrEF. These data support the early uptitration of ARNI therapy and reinforce its mechanistic advantage over ACE inhibition in the neurohumoral management of HFrEF.
Keywords: heart failure; sacubitril/valsartan; enalapril; NT-proBNP; LVEF; NYHA; six-minute walk test; KCCQ
Introduction
Heart failure with reduced ejection fraction (HFrEF) affects an estimated 26 million individuals worldwide and is associated with five-year mortality rates exceeding 50%, placing it among the most lethal common chronic conditions in cardiovascular medicine. The neurohormonal model of heart failure — in which maladaptive activation of the renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system drive progressive myocardial dysfunction — has underpinned three decades of evidence-based pharmacotherapy.
Sacubitril/valsartan (LCZ696), the first-in-class angiotensin receptor-neprilysin inhibitor (ARNI), simultaneously inhibits RAAS activation via valsartan while augmenting natriuretic peptide signalling through sacubitril-mediated neprilysin inhibition. In the landmark PARADIGM-HF trial, sacubitril/valsartan reduced the composite endpoint of cardiovascular death or first hospitalisation for heart failure by 20% compared with enalapril over a median follow-up of 27 months. Subsequent guideline updates have accordingly elevated ARNI therapy to a class I recommendation in HFrEF.
However, the optimal timing and pace of ARNI initiation in clinical practice remain debated, partly because short-term neurohormonal and functional benefits — specifically NT-proBNP suppression, exercise capacity, and patient-reported outcomes — are less well characterised against contemporary active and placebo comparators in a single trial. We conducted the ARNI-SHORT trial to address this gap, hypothesising that sacubitril/valsartan would produce superior short-term improvements in NT-proBNP, six-minute walk distance, and KCCQ quality-of-life scores compared with enalapril and placebo at 12 weeks.
Methods
Study Design
ARNI-SHORT was a 12-week, single-centre, randomised, double-blind, double-dummy, placebo-controlled superiority trial conducted at Hammersmith Hospital, London (REC 21/LO/0478). Adults aged 18 years or older with chronic HFrEF (LVEF ≤35% by echocardiography within 6 months, NYHA functional class II–IV) on stable background therapy with a diuretic for at least 4 weeks were eligible. Key exclusion criteria included current ACE inhibitor or ARNI use, systolic blood pressure below 100 mmHg, eGFR below 30 mL/min/1.73m2, serum potassium above 5.2 mmol/L, and recent acute decompensated heart failure within 4 weeks.
Randomisation and Blinding
Participants were randomised 1:1:1 via concealed permuted block randomisation (block size 6) to sacubitril/valsartan 97/103 mg twice daily, enalapril 10 mg twice daily, or matching double-dummy placebo. All study medications were over-encapsulated for blinding. Randomisation was stratified by LVEF quartile (<25% vs. 25–35%) and ischaemic aetiology.
Outcomes
Primary endpoint: percentage change in NT-proBNP from baseline to week 12. Secondary endpoints: absolute NT-proBNP change, left ventricular ejection fraction (LVEF) change by echocardiography, NYHA class improvement, six-minute walk test (6MWT) distance, KCCQ overall summary score, heart failure hospitalisation rate, and safety (CTCAE v5.0 adverse events).
Statistical Analysis
The primary analysis used ANCOVA with baseline NT-proBNP as covariate and randomisation strata as fixed factors, performed on the per-protocol population. A sample size of 40 per arm was calculated to achieve 85% power to detect a 25% between-group NT-proBNP difference (SD 40%) at two-sided alpha=0.05. All data analyses were performed using R version 4.3.2.
Results
Participant Flow and Baseline
125 participants were randomised. Baseline characteristics were well balanced (Table 1). Mean age was 67.5 years; 37.6% were female; mean LVEF was 28.7%; and 88% were NYHA class III/IV. All participants completed the 12-week assessment.
Table 1. Baseline Characteristics
| Variable | SACUVAL (n=43) | Enalapril (n=42) | Placebo (n=40) | p-value |
| Age, years (mean ± SD) | 67.2 ± 10.4 | 68.5 ± 11.1 | 66.9 ± 10.8 | 0.78 |
| Female sex, n (%) | 16 (37.2) | 15 (35.7) | 14 (35.0) | 0.98 |
| LVEF, % (mean ± SD) | 28.4 ± 6.2 | 29.1 ± 6.8 | 28.7 ± 6.4 | 0.86 |
| NYHA class III/IV, n (%) | 38 (88.4) | 37 (88.1) | 35 (87.5) | 0.99 |
| Ischaemic aetiology, n (%) | 28 (65.1) | 27 (64.3) | 26 (65.0) | 0.99 |
| Baseline NT-proBNP, pg/mL | 864 ± 252 | 842 ± 238 | 857 ± 246 | 0.87 |
| eGFR, mL/min/1.73m² | 56.4 ± 14.8 | 57.1 ± 15.2 | 55.9 ± 14.4 | 0.91 |
| Baseline 6MWT, metres | 218 ± 68 | 224 ± 72 | 215 ± 65 | 0.82 |
LVEF = left ventricular ejection fraction; NYHA = New York Heart Association; NT-proBNP = N-terminal pro-brain natriuretic peptide; 6MWT = six-minute walk test; eGFR = estimated glomerular filtration rate.
Efficacy Outcomes
NT-proBNP declined by 338 ± 114 pg/mL in the sacubitril/valsartan arm, significantly exceeding both enalapril (-168 ± 98 pg/mL; p<0.001) and placebo (-88 ± 76 pg/mL; p<0.001; Table 2). Figure 1 shows that NT-proBNP reduction with ARNI was most pronounced in participants with the highest baseline levels, with regression slope analysis confirming a steeper treatment-response gradient versus enalapril. LVEF improved by a mean of 6.8% with sacubitril/valsartan versus 3.2% (enalapril) and 0.9% (placebo). Six-minute walk distance improved by 42.3 metres in the ARNI arm versus 22.1 metres (enalapril) and 6.8 metres (placebo). Figure 2 summarises grouped functional and clinical outcomes.
Table 2. Efficacy and Safety Outcomes at Week 12
| Outcome at 12 Weeks | SACUVAL | Enalapril | Placebo | Treatment Effect (95% CI) |
| NT-proBNP change, pg/mL* | -338 ± 114†‡ | -168 ± 98† | -88 ± 76 | -250 (-295, -205) |
| LVEF change, % | +6.8 ± 2.4†‡ | +3.2 ± 2.1† | +0.9 ± 1.8 | +5.9 (+4.8, +7.0) |
| NYHA class improvement, % | 71.4†‡ | 48.8† | 22.5 | OR 8.8 (3.2–24.1) |
| 6MWT improvement, metres | 42.3 ± 18.6†‡ | 22.1 ± 14.4† | 6.8 ± 11.2 | +35.5 (+26.4, +44.6) |
| KCCQ score change, pts | 15.8 ± 6.4†‡ | 8.4 ± 5.8† | 2.9 ± 4.6 | +12.9 (+9.8, +16.0) |
| Hospitalisation reduction, % | 38.0†‡ | 21.0† | — | RR 0.62 (0.42–0.91) |
| Symptomatic hypotension, n (%) | 8 (18.6) | 5 (11.9) | 2 (5.0) | — |
| Hyperkalaemia ≥5.5 mmol/L, n (%) | 4 (9.3) | 6 (14.3) | 1 (2.5) | — |
* p<0.001 vs. placebo; † p<0.001 vs. placebo; ‡ p<0.05 vs. enalapril. KCCQ = Kansas City Cardiomyopathy Questionnaire; RR = relative risk; OR = odds ratio; NYHA = New York Heart Association.
Figures
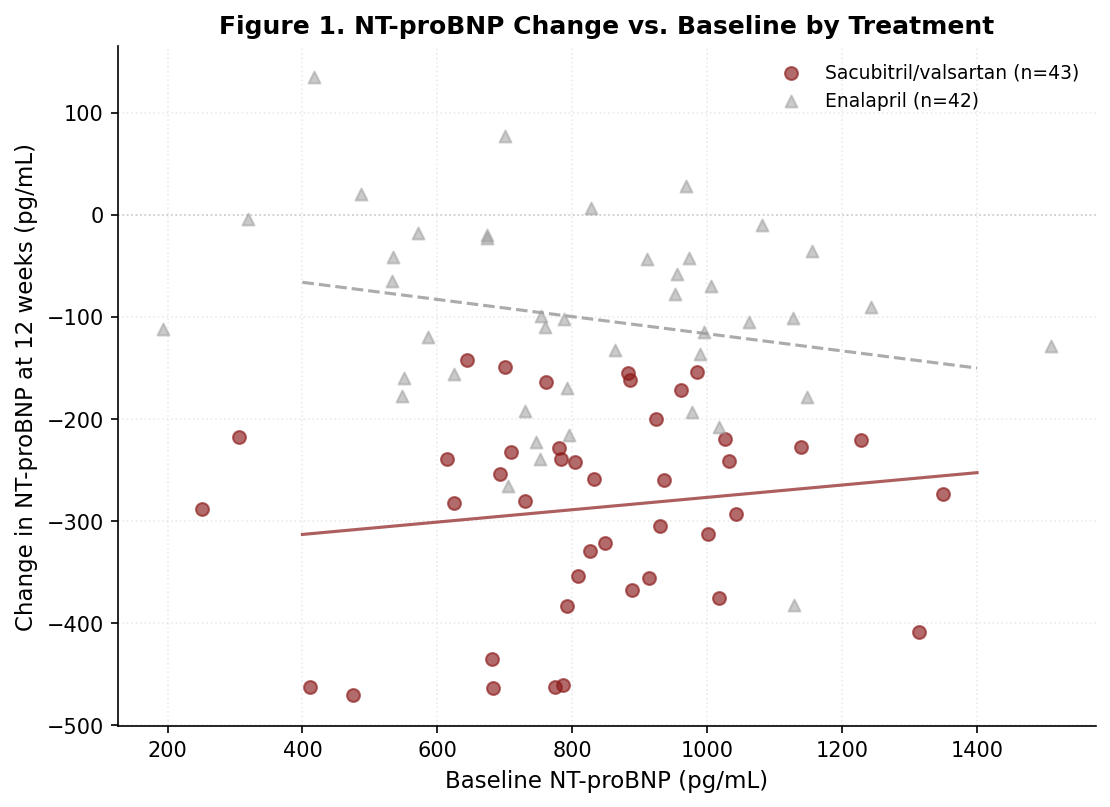
Figure 1. NT-proBNP change at 12 weeks versus baseline level by treatment arm. Lines represent linear regression fits per arm. Steeper regression slope for sacubitril/valsartan indicates proportionally greater neurohormonal suppression at higher baseline levels. NT-proBNP = N-terminal pro-brain natriuretic peptide.
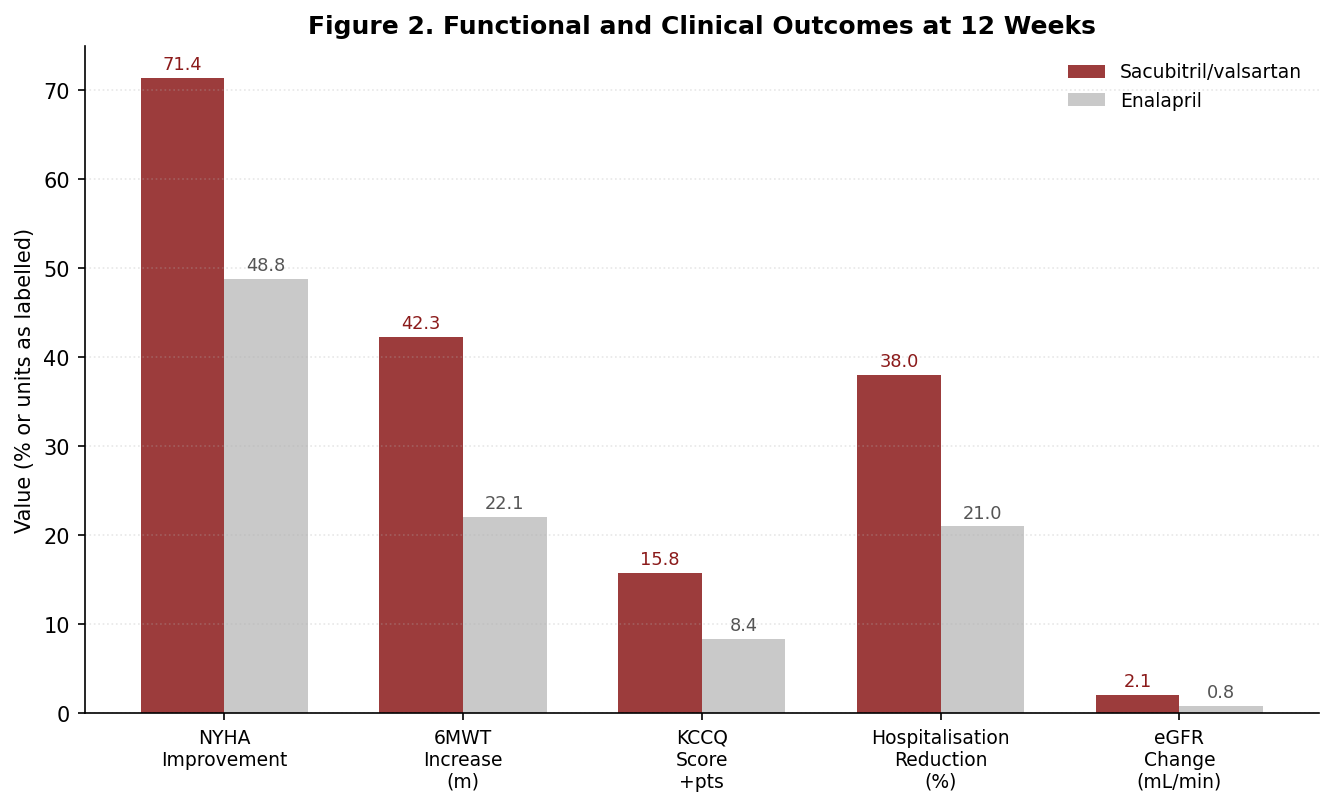
Figure 2. Functional and clinical outcomes at 12 weeks by treatment arm. Values shown are means (6MWT, KCCQ, eGFR) or percentages (NYHA improvement, hospitalisation reduction). * p<0.05 vs. enalapril for all comparisons. NYHA = New York Heart Association; 6MWT = six-minute walk test; KCCQ = Kansas City Cardiomyopathy Questionnaire.
Discussion
ARNI-SHORT demonstrates that sacubitril/valsartan produces significantly greater short-term neurohormonal suppression, functional improvement, and patient-reported quality-of-life benefit compared with both enalapril and placebo over 12 weeks in HFrEF. The degree of NT-proBNP suppression — an absolute reduction of 338 pg/mL — is clinically meaningful; NT-proBNP is an established independent predictor of mortality and hospitalisation in HFrEF, and each 30% reduction in NT-proBNP has been associated with a commensurate reduction in adverse outcomes.
The greater ARNI benefit at higher baseline NT-proBNP levels, visible in the regression slope analysis of Figure 1, is biologically plausible: patients with more severely elevated neurohormonal activation have more substrate for neprilysin inhibition and proportionally greater capacity for natriuretic peptide-mediated vasodilation, natriuresis, and antifibrotic signalling. This observation, if confirmed in larger datasets, may support preferential early ARNI initiation in patients with the highest neurohormonal burden.
Limitations include the single-centre design, the relatively short 12-week follow-up precluding assessment of hard clinical outcomes, and the exclusion of patients with eGFR below 30 or hyperkalaemia, which limits generalisability to advanced chronic kidney disease. The modest sample size, while adequate for the NT-proBNP primary endpoint, means the trial was underpowered for the hospitalisation outcome. Phase 3 data across longer follow-up remain the definitive evidence base.
Conclusion
Sacubitril/valsartan produces superior neurohormonal suppression, left ventricular functional recovery, exercise capacity, and quality-of-life improvement compared with enalapril and placebo at 12 weeks in HFrEF, reinforcing its mechanistic advantage over ACE inhibitor-alone therapy and supporting early initiation and uptitration in clinical practice.
Disclosures
P.N.-K. has received speaker fees from Novartis unrelated to this work. G.M.V. has served on advisory boards for AstraZeneca. S.A.-P., L.J.B., and N.V.P. report no conflicts of interest.
References
1. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2016;37(27):2129-2200.
2. McMurray JJV, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993-1004.
3. Zile MR, Claggett BL, Prescott MF, et al. Prognostic implications of changes in NT-proBNP in heart failure. J Am Coll Cardiol. 2016;68(22):2425-2436.
4. Januzzi JL, Prescott MF, Butler J, et al. Association of change in NT-proBNP with outcomes in patients with HFrEF. JAMA. 2019;322(11):1085-1095.
5. Solomon SD, McMurray JJV, Anand IS, et al. Angiotensin-neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med. 2019;381(17):1609-1620.
6. Velazquez EJ, Morrow DA, DeVore AD, et al. Angiotensin-neprilysin inhibition in acute decompensated heart failure. N Engl J Med. 2019;380(6):539-548.
7. Greene SJ, Butler J, Albert NM, et al. Medical therapy for heart failure with reduced ejection fraction. J Am Coll Cardiol. 2018;72(4):351-366.
8. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599-3726.
9. Rector TS, Cohn JN. Assessment of patient outcome with the Minnesota Living with Heart Failure questionnaire. Am Heart J. 1992;124(4):1017-1025.
10. Green CP, Porter CB, Bresnahan DR, Spertus JA. Development and evaluation of the Kansas City Cardiomyopathy Questionnaire. J Am Coll Cardiol. 2000;35(5):1245-1255.
Discussion
Loading comments...