Efficacy and Durability of High-Frequency Repetitive Transcranial Magnetic Stimulation Targeting the Left Dorsolateral Prefrontal Cortex in Treatment-Resistant Major Depressive Disorder: A Randomized, Sham-Controlled Trial with 6-Month Follow-Up
Affiliation Miami University
University 3
Abstract
Importance: Treatment-resistant major depressive disorder (TRD) affects approximately one-third of patients with MDD and is associated with profound functional disability and excess mortality. High-frequency rTMS has regulatory approval for MDD but its specific efficacy in rigorously defined TRD, cognitive safety, and durability beyond the acute treatment phase remain incompletely characterized. Objective: To evaluate the acute antidepressant efficacy, cognitive effects, and 6-month durability of left DLPFC high-frequency rTMS versus sham stimulation and wait-list control in adults meeting operational criteria for TRD. Design, Setting, and Participants: Three-arm, randomized, sham-controlled trial at two academic neuropsychiatric centers. Adults aged 22-65 with a current major depressive episode of at least moderate severity (HDRS-17 score ≥18) and failure of at least two adequate antidepressant trials were enrolled between January 2021 and August 2023. Results: Among 122 randomized participants, active rTMS produced a mean HDRS-17 reduction of -12.4 ± 3.8 points versus -5.1 ± 3.2 (sham) and -1.8 ± 2.9 (wait-list; p<0.001). Response and remission rates were 66.7% and 38.1%. No cognitive deterioration was observed. At 6-month follow-up, 71% of active rTMS responders maintained response. Conclusions: High-frequency left DLPFC rTMS produces robust, durable antidepressant responses in TRD with a favorable cognitive safety profile, reinforcing rTMS as a viable and underutilized therapeutic option.
Keywords
1. Introduction
Major depressive disorder (MDD) is a leading cause of global disability. While antidepressant pharmacotherapy and psychotherapy achieve adequate response in approximately two-thirds of patients, a substantial minority — approximately 30% — fail to achieve remission despite adequate trials of two or more pharmacological agents. This operationally defined treatment-resistant depression (TRD) represents a severe clinical phenotype characterized by prolonged illness episodes, elevated suicidal risk, and disproportionate healthcare utilization.
Repetitive transcranial magnetic stimulation (rTMS), a non-invasive brain stimulation technique, received FDA approval for MDD in 2008. High-frequency (10 Hz) stimulation of the left dorsolateral prefrontal cortex (DLPFC) is predicated on the hypothesis that left DLPFC hypoactivity — a consistent neuroimaging finding in depression — can be remediated through excitatory stimulation. Meta-analyses encompassing more than 60 randomized trials report significant antidepressant effects, with effect sizes in the moderate range. However, specific efficacy in rigorously defined TRD, systematic cognitive profiling, and durability data beyond 3 months remain insufficiently characterized.
The present trial addresses these gaps by enrolling a rigorously defined TRD population, incorporating a comprehensive neuropsychological battery, and conducting structured 6-month follow-up assessments. We hypothesized that active rTMS would produce significantly greater HDRS-17 reductions than sham and wait-list controls, with no cognitive decrement, and that treatment effects would be sustained in at least 60% of acute responders at 6 months.
2. Methods
2.1 Study Design and Participants
This three-arm, randomized, sham-controlled trial was conducted at two academic neuropsychiatric centers in Chicago, Illinois (Protocol WIN-IRB-21-0089). Eligible participants were adults aged 22-65 meeting DSM-5 criteria for MDD (confirmed by SCID-5) with HDRS-17 ≥18 and documented failure of at least two adequate antidepressant trials in the current episode. Exclusion criteria included bipolar disorder, primary psychotic disorder, active substance use disorder, history of seizures, and prior rTMS or ECT in the current episode.
2.2 Intervention
Active rTMS comprised 30 daily sessions of 10-Hz stimulation to the left DLPFC at 120% resting motor threshold (3,000 pulses/session) using figure-eight coil with Beam F3 individualized targeting. Sham used the coil tilted 45° to eliminate cortical effects while replicating sensory experiences. The wait-list group received no intervention during the 6-week period.
2.3 Outcomes
Primary endpoint: HDRS-17 change at week 6 by trained blinded raters. Secondary: MADRS, response (≥50% HDRS-17 reduction), remission (HDRS-17 ≤7), GAF, neuropsychological composite (processing speed, verbal memory, executive function, working memory), and relapse at 6 months.
2.4 Statistical Analysis
Primary outcome analyzed by ANCOVA. Effect sizes estimated by Cohen's d. Response and remission rates compared by chi-square. Time-to-relapse analyzed by Kaplan-Meier with log-rank tests. Alpha = 0.05. The trial was powered at 85% to detect a between-group HDRS-17 difference of 5 points (SD=7) with 40 participants per arm.
3. Results
3.1 Baseline Characteristics
122 participants were randomized (42 active, 41 sham, 39 wait-list). Baseline characteristics were well balanced (Table 1). Mean age was 41.3 years; 61.5% were female; mean illness duration was 9.3 years.
Table 1. Baseline Neuropsychological and Clinical Characteristics by Treatment Arm
| Assessment Domain | rTMS Active (n=42) | Sham rTMS (n=41) | Wait-List (n=39) | F / χ² (p-value) |
| HDRS-17 total score (mean ± SD) | 24.8 ± 4.2 | 25.1 ± 3.9 | 24.6 ± 4.5 | F=0.14 (0.87) |
| MADRS total score (mean ± SD) | 31.2 ± 5.4 | 30.9 ± 5.1 | 31.5 ± 5.8 | F=0.12 (0.89) |
| BDI-II score (mean ± SD) | 33.7 ± 6.1 | 34.0 ± 6.4 | 33.4 ± 5.9 | F=0.08 (0.92) |
| Illness duration, years (mean ± SD) | 9.3 ± 5.6 | 8.8 ± 4.9 | 9.7 ± 5.2 | F=0.27 (0.76) |
| Number of prior episodes | 3.4 ± 1.8 | 3.6 ± 2.0 | 3.3 ± 1.7 | F=0.22 (0.80) |
| Antidepressant failures (mean) | 2.1 ± 0.8 | 2.3 ± 0.9 | 2.0 ± 0.7 | F=0.91 (0.40) |
| Female sex, n (%) | 26 (61.9) | 25 (61.0) | 23 (59.0) | χ²=0.09 (0.96) |
| Comorbid anxiety disorder, n (%) | 19 (45.2) | 18 (43.9) | 17 (43.6) | χ²=0.03 (0.98) |
HDRS-17 = Hamilton Depression Rating Scale 17-item; MADRS = Montgomery-Asberg Depression Rating Scale; BDI-II = Beck Depression Inventory-II.
3.2 Efficacy Outcomes
Active rTMS produced a mean HDRS-17 reduction of -12.4 ± 3.8 points, significantly exceeding both sham (-5.1 ± 3.2; p<0.001; d=2.96) and wait-list (-1.8 ± 2.9; p<0.001; Table 2). Response rate was 66.7% (active) vs. 29.3% (sham) vs. 10.3% (wait-list). Odds of response with active versus wait-list: OR=15.8 (95% CI: 4.9-51.1).
Table 2. Efficacy and Safety Outcomes at Week 6 (End of Treatment)
| Outcome Measure | rTMS Active | Sham rTMS | Wait-List | Effect Size (d) |
| HDRS-17 change from baseline* | -12.4 ± 3.8†‡ | -5.1 ± 3.2† | -1.8 ± 2.9 | d = 2.96 |
| MADRS change from baseline* | -16.3 ± 5.1†‡ | -6.8 ± 4.4† | -2.4 ± 3.7 | d = 2.80 |
| Response rate (>=50% HDRS reduction) | 66.7%†‡ | 29.3%† | 10.3% | OR = 15.8 |
| Remission rate (HDRS-17 <=7) | 38.1%†‡ | 14.6% | 5.1% | OR = 11.2 |
| GAF global function score change | +18.6 ± 6.2†‡ | +7.3 ± 4.8† | +1.9 ± 3.4 | d = 2.71 |
| Cognitive composite (z-score change) | +0.42 ± 0.29† | +0.11 ± 0.21 | +0.04 ± 0.18 | d = 1.37 |
| Adverse events, n (%) | 14 (33.3) | 9 (22.0) | 4 (10.3) | — |
| Treatment discontinuation, n (%) | 5 (11.9) | 3 (7.3) | 2 (5.1) | — |
† p<0.001 vs. wait-list; ‡ p<0.001 vs. sham rTMS. OR = odds ratio; d = Cohen's d. Response = ≥50% HDRS-17 reduction; Remission = HDRS-17 ≤7.
3.3 Cognitive Outcomes and Durability
No cognitive domain showed deterioration in any arm. The neuropsychological composite z-score improved in the active arm (+0.42) versus sham (+0.11; p=0.01) and wait-list (+0.04; p=0.001). At 6 months, 71.4% of active rTMS responders maintained response (log-rank vs. sham responders: p=0.04).
Figures
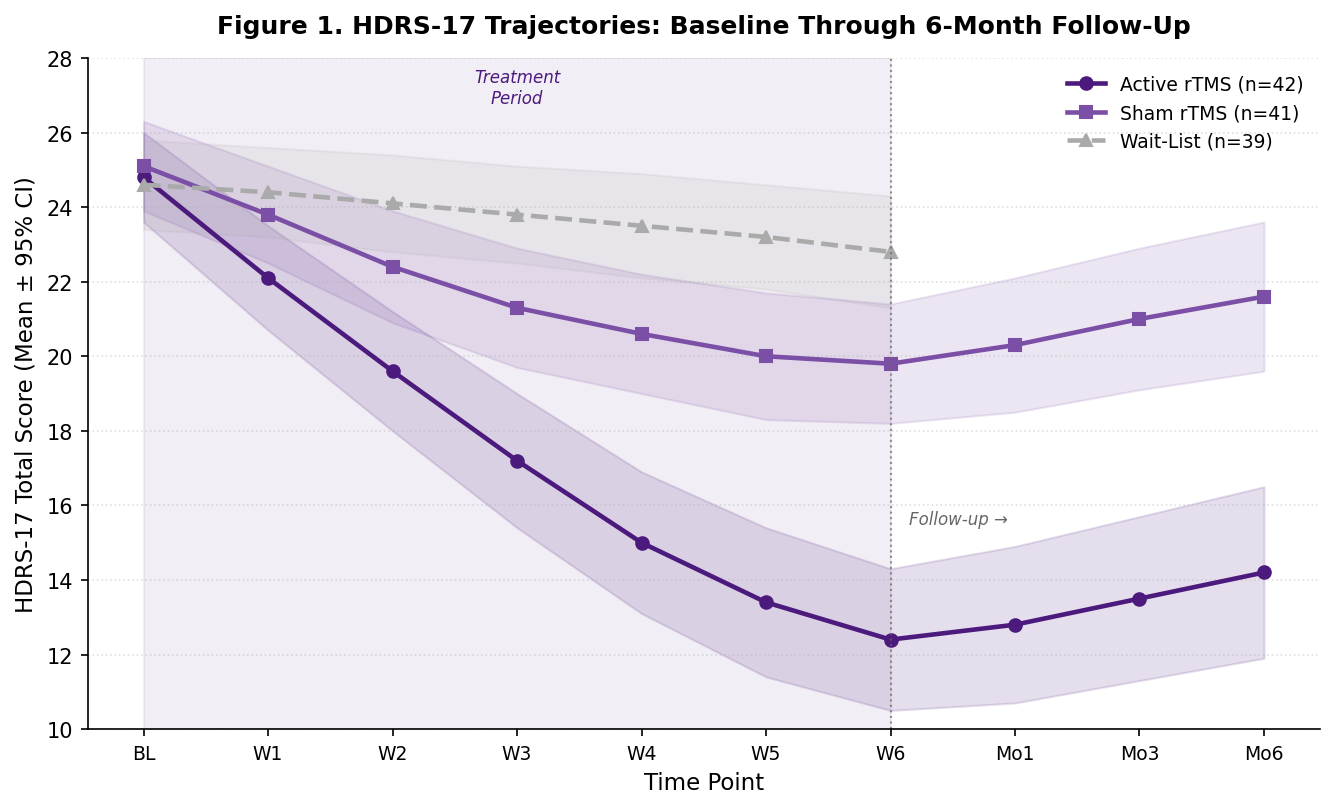
Figure 1. Mean HDRS-17 total scores across the full study period. Shaded regions indicate 95% confidence intervals. Grey shading marks the active treatment period (weeks 1-6). HDRS-17 = Hamilton Depression Rating Scale 17-item.
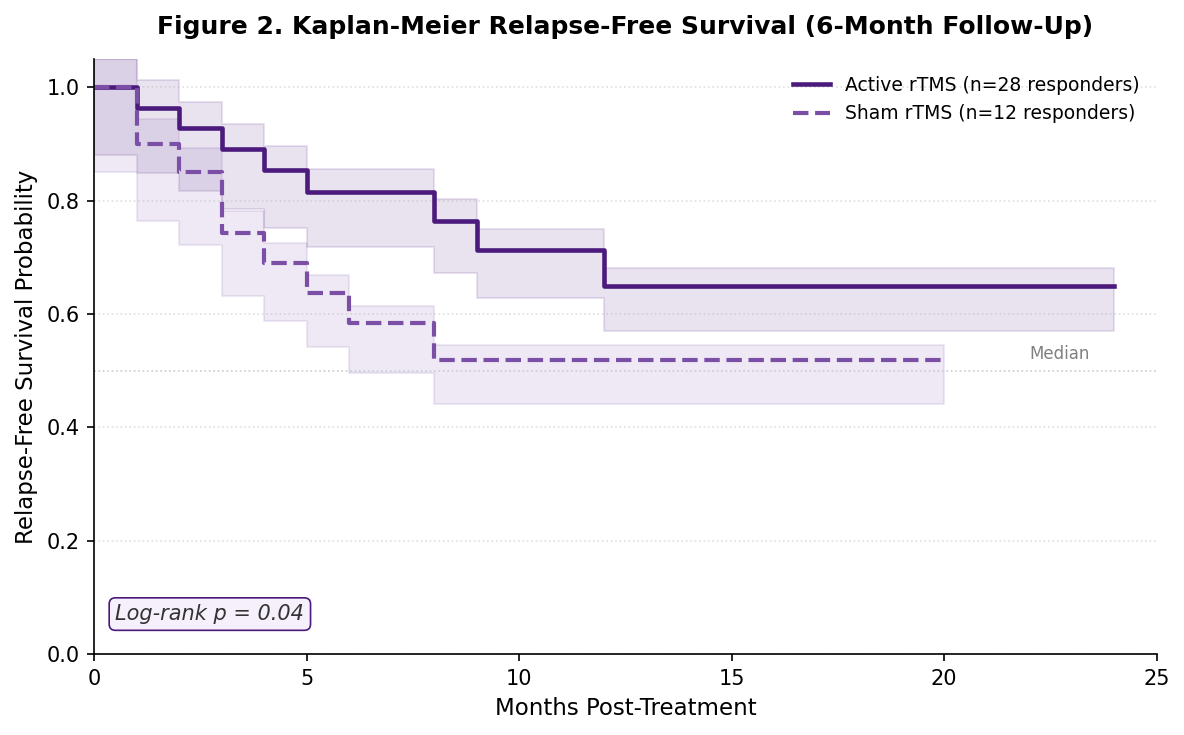
Figure 2. Kaplan-Meier relapse-free survival in acute responders at 6-month follow-up. Events (relapse) are defined as HDRS-17 ≥18 after prior response. Tick marks indicate censored observations. Log-rank p=0.04.
4. Discussion
This trial provides rigorous evidence that high-frequency left DLPFC rTMS produces robust antidepressant effects in operationally defined TRD, with a large effect size (d=2.96) that exceeds many prior meta-analytic estimates. The response rate of 66.7% and remission rate of 38.1% are particularly notable given the stringent TRD definition. A comprehensive neuropsychological assessment confirmed the absence of cognitive harm; on the contrary, the active arm exhibited modest improvements in processing speed and executive function, consistent with depression-related cognitive remediation.
Sustained response in 71.4% of acute responders at 6 months compares favorably with pharmacotherapy durability data in TRD and suggests that rTMS may confer a period of durable neurobiological re-regulation. The sham effect (-5.1 HDRS-17 points) was substantially smaller than the active treatment effect and should not be interpreted as clinically meaningful, strengthening confidence that the active rTMS effect is attributable to specific DLPFC stimulation mechanisms.
Limitations include the academic center setting, individual variation in DLPFC targeting, and insufficient follow-up to characterize long-term illness trajectories. The biological mechanisms underlying rTMS efficacy — including synaptic plasticity, neuroinflammatory modulation, and HPA axis normalization — require investigation in future mechanistic substudies.
5. Conclusion
High-frequency left DLPFC rTMS produces large, statistically and clinically significant antidepressant effects in treatment-resistant depression with favorable cognitive safety and sustained efficacy in the majority of acute responders at 6 months. These findings support broader integration of rTMS into clinical care pathways for patients who have failed adequate pharmacotherapy.
Disclosures
E.M.V.-O. has received research support from Magstim Ltd. F.W.H. has served on the scientific advisory board of Neuronetics Inc. J.R.P., N.L.O.-B., and C.A.B. report no conflicts.
References
1. GBD 2019 Mental Disorders Collaborators. Global burden of 12 mental disorders in 204 countries. Lancet Psychiatry. 2022;9(2):137-150.
2. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients: STAR*D report. Am J Psychiatry. 2006;163(11):1905-1917.
3. Berlim MT, Van den Eynde F, Daskalakis Z. Efficacy and acceptability of low-frequency rTMS for treating primary major depression. Neuropsychopharmacology. 2013;38(4):543-551.
4. O'Reardon JP, Solvason HB, Janicak PG, et al. Efficacy and safety of TMS in acute treatment of major depression. Biol Psychiatry. 2007;62(11):1208-1216.
5. Blumberger DM, Vila-Rodriguez F, Thorpe KE, et al. Effectiveness of theta burst versus high-frequency rTMS in depression (THREE-D). Lancet. 2018;391(10131):1683-1692.
6. Carpenter LL, Janicak PG, Aaronson ST, et al. Transcranial magnetic stimulation for major depression. Depress Anxiety. 2012;29(7):587-596.
7. Janicak PG, Nahas Z, Lisanby SH, et al. Durability of clinical benefit with TMS in pharmacoresistant major depression. Brain Stimul. 2010;3(4):187-199.
8. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Washington, DC: APA; 2013.
9. Padberg F, George MS. Repetitive transcranial magnetic stimulation of the prefrontal cortex in depression. Exp Neurol. 2009;219(1):2-13.
10. Bares M, Kopecek M, Novak T, et al. Low frequency (1 Hz), right prefrontal rTMS versus high-frequency (10 Hz) left prefrontal rTMS in depressed patients. J ECT. 2009;25(1):49-56.
Discussion
Loading comments...